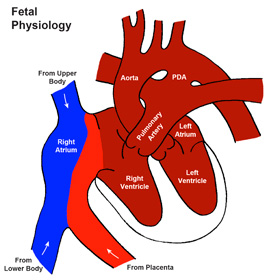
 The physiology of the heart and vascular system changes dramatically around the time of birth. Prior to birth, the heart works in concert with the mother’s placenta to provide oxygen rich blood to the body of the baby. Before a baby is born, very little blood sent to the lungs, most is diverted away from the lungs through a vessel called the ductus arteriosus. Before birth, the ductus arteriosus is as large as the aorta.
The physiology of the heart and vascular system changes dramatically around the time of birth. Prior to birth, the heart works in concert with the mother’s placenta to provide oxygen rich blood to the body of the baby. Before a baby is born, very little blood sent to the lungs, most is diverted away from the lungs through a vessel called the ductus arteriosus. Before birth, the ductus arteriosus is as large as the aorta.
Not all of the blood pumped from the fetal heart is sent to the placenta to collect oxygen either. Before birth, the typical oxygen saturation in a normal fetus is between 65% and 70%.
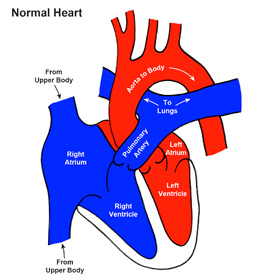
At the time of delivery, the physiology of the heart and vascular system changes so that the lungs become the source of oxygen for the baby. When all goes well, the transition goes smoothly and the ductus arteriosus closes within the first day or two. In a normal baby, once the ductus arteriosus closes, the blood which is low in oxygen returning from the body is separated from the oxygen rich blood returning from the lungs.
When there are anatomic problems with the baby’s heart, the normal transition may be delayed, potentially masking the severity of the heart defect. The term “ductal dependent” heart defects are those in which the ductus arteriosus is necessary to allow blood to flow to either the lungs or the body.
The development is the fetal heart is fantastically complicated and is largely completed by the 9th week of pregnancy. As it turns out, there are many situations in which a malformed heart will function adequately in fetal life, but will not be successful after birth when the transition in physiology is complete and the ductus arteriosus closes.