
The Centers for Disease Control and Prevention (CDC) and the American Academy of Pediatrics (AAP) are trusted sources for the best practices to keep kids safe during the Covid-19 pandemic. These two organizations agree on a layered approach to reducing Covid-19 spread to and amongst children, including correct mask use, physical distancing, screening, ventilation, hand washing and respiratory etiquette, cleaning and disinfection, vaccination for eligible persons, and staying home when sick. The Department of Pediatrics stands in strong agreement with the CDC and AAP guidance. This agreement should reassure families. That said, we understand that misinformation about masking and prevention protocols is concerning to parents. Below, we address the top myths about Covid-19 and children, and we provide a list of trusted resources and sites for accurate information about fostering the health and well-being of all children in Wisconsin.
Children and Covid-19: State-Level Data Report
State-level reports are the best publicly available and timely data on child Covid-19 cases in the United States. The American Academy of Pediatrics and the Children’s Hospital Association are collaborating to collect and share all publicly available data from states on child Covid-19 cases. View the latest report.
Myths about Covid and Kids
This is an accordion element with a series of buttons that open and close related content panels.
Myth #1: Kids don’t get seriously sick from Covid-19.
FACT: Children and adolescents can be infected with SARS-CoV-2, can get sick with Covid-19, and can spread the virus to others.
| While children do not die from the virus at the same rate as adults, they can still die from COVID-19, they can still get very sick, and some get sick enough to be hospitalized. In fact, children die from COVID-19 at rates similar to other diseases for which children are vaccinated or kept out of school. |
| Several studies conducted early during the COVID-19 pandemic suggested that the incidence rate among children and adolescents was lower than among adults. However, the lower incidence rates may have been due in part to children, when compared to adults, having fewer opportunities for exposure (due to school, daycare, and activity closures) and a lower probability of being tested. |
| Children can transmit the virus to others, which is especially dangerous for families that include someone who is immunocompromised. In fact, some children are at higher risk of COVID-19 due to medical conditions. |
| As of July 2021, more than 4,000 children with COVID-19 developed multisystem inflammatory syndrome and more than 340 children have died from COVID-19 in the United States. It is notable that this impact was documented when many mitigating measures were in place across the country and therefore, may not represent the potential full impact on children. |
| In addition to deaths and severe illness, some children develop long-Covid symptoms and other complications due to infection with SARS-CoV-2. Researchers are just beginning to understand the longer-term impacts that even mild Covid infections may have on children. |
| As of July 2021, more than 40,000 children in the United States have lost a parent to Covid-19, and it is estimated that more than 120,000 have lost a primary caregiver. |
Myth #2: Masks don’t work.
FACT: Studies have shown that universal masking has been an incredibly effective tool for controlling the spread of Covid-19 in schools.
| Universal masking can allow schools to largely operate normally. |
| Distancing can be reduced in the classroom or on the bus when everyone is masked. |
| If children are exposed to Covid-19 in a fully masked environment, they do not need to quarantine. |
| Most children can mask successfully, few children with specific needs may need accommodations if they are unable to consistently mask. |
Here are a few studies that have shown how layered prevention strategies can be successful in limiting transmission in schools:
| Zimmerman KO, Akinboyo IC, Brookhart MA, et al. Incidence and Secondary Transmission of SARS-CoV-2 Infections in Schools. Pediatrics 2021;147(4). doi:10.1542/peds.2020-048090 |
| Volpp KG, Kraut BH, Ghosh S, et al. Minimal SARS-CoV-2 Transmission After Implementation of a Comprehensive Mitigation Strategy at a School – New Jersey, August 20-November 27, 2020. MMWR Morb Mortal Wkly Rep 2021;70(11):377-381. doi:10.15585/mmwr.mm7011a2 |
| Link-Gelles R, DellaGrotta AL, Molina C, et al. Limited Secondary Transmission of SARS-CoV-2 in Child Care Programs – Rhode Island, June 1-July 31, 2020. MMWR Morb Mortal Wkly Rep 2020;69(34):1170-1172. doi:10.15585/mmwr.mm6934e2 |
| Gandini S, Rainisio M, Iannuzzo ML, et al. A cross-sectional and prospective cohort study of the role of schools in the SARS-CoV-2 second wave in Italy. Lancet Reg Health Eur 2021;5:100092. doi:10.1016/j.lanepe.2021.100092 |
| Fricchione MJ, Seo JY, Arwady MA. Data-Driven Reopening of Urban Public Education Through Chicago’s Tracking of COVID-19 School Transmission. J Public Health Manag Pract 2021;27(3):229-232. doi:10.1097/phh.0000000000001334 |
| Kim C, McGee S, Khuntia S, et al. Characteristics of COVID-19 Cases and Outbreaks at Child Care Facilities – District of Columbia, July-December 2020. MMWR Morb Mortal Wkly Rep 2021;70(20):744-748. doi:10.15585/mmwr.mm7020a3 |
For how inconsistent mask use may have contributed to school-based outbreaks, check out:
| Stein-Zamir C, Abramson N, Shoob H, et al. A large COVID-19 outbreak in a high school 10 days after schools’ reopening, Israel, May 2020. Euro Surveill 2020;25(29)doi:10.2807/1560-7917.Es.2020.25.29.2001352 |
| Gold JA, Gettings JR, Kimball A, et al. Clusters of SARS-CoV-2 Infection Among Elementary School Educators and Students in One School District — Georgia, December 2020–January 2021. MMWR Morb Mortal Wkly 2021;70:289-292. doi:10.15585/mmwr.mm7008e4 |
Myth #3: Masks can be dangerous to kids (e.g., masks restrict air flow, increase CO2 levels in the bloodstream, cause CO2 poisoning).
FACT: Masks are made of breathable material that does not block oxygen or trap CO2.
| Mask are designed to reduce respiratory droplets that may contain Covid-19, either from the wearer or to protect the wearer from others, but oxygen can flow through and around the mask. |
| CO2 molecules are so small, they flow through masks like oxygen. |
| Proper masks are safe for kids. |
| Children under the age of two, those with special needs, cognitive impairments or severe breathing problems should not wear a mask for their safety and caregivers should consult their pediatrician for guidance on Covid-19 prevention. |
Myth #4: Vaccines for teens were rushed and are not safe.
FACT: Vaccines are extremely effective and have been extensively tested to show that they are safe.
| As of July 2021, more than four billion people have received at least one dose of a COVID vaccine and more than a billion people are fully vaccinated worldwide. Serious side effects are extremely rare. |
| All vaccines that are approved for children and teens go through the same testing and review as those developed for adults. |
| The FDA is continuously monitoring for unusual side effects even after vaccines are authorized. All reports are taken seriously and investigated thoroughly. |
| Studies of COVID-19 vaccines in children <12 years of age are ongoing, but approval will not occur until there are sufficient data that proves they are safe and effective. It will take some time until vaccines are available for these younger age groups. |
Trusted Information

American Academy of Pediatrics
Read the American Academy of Pediatrics' Covid-19 Guidance for Safe Schools.

Centers for Disease Control & Prevention (CDC)
Read the CDC's science brief on transmission of SARS-CoV-2 in K-12 schools and early childcare programs.
Your Local Epidemiologist
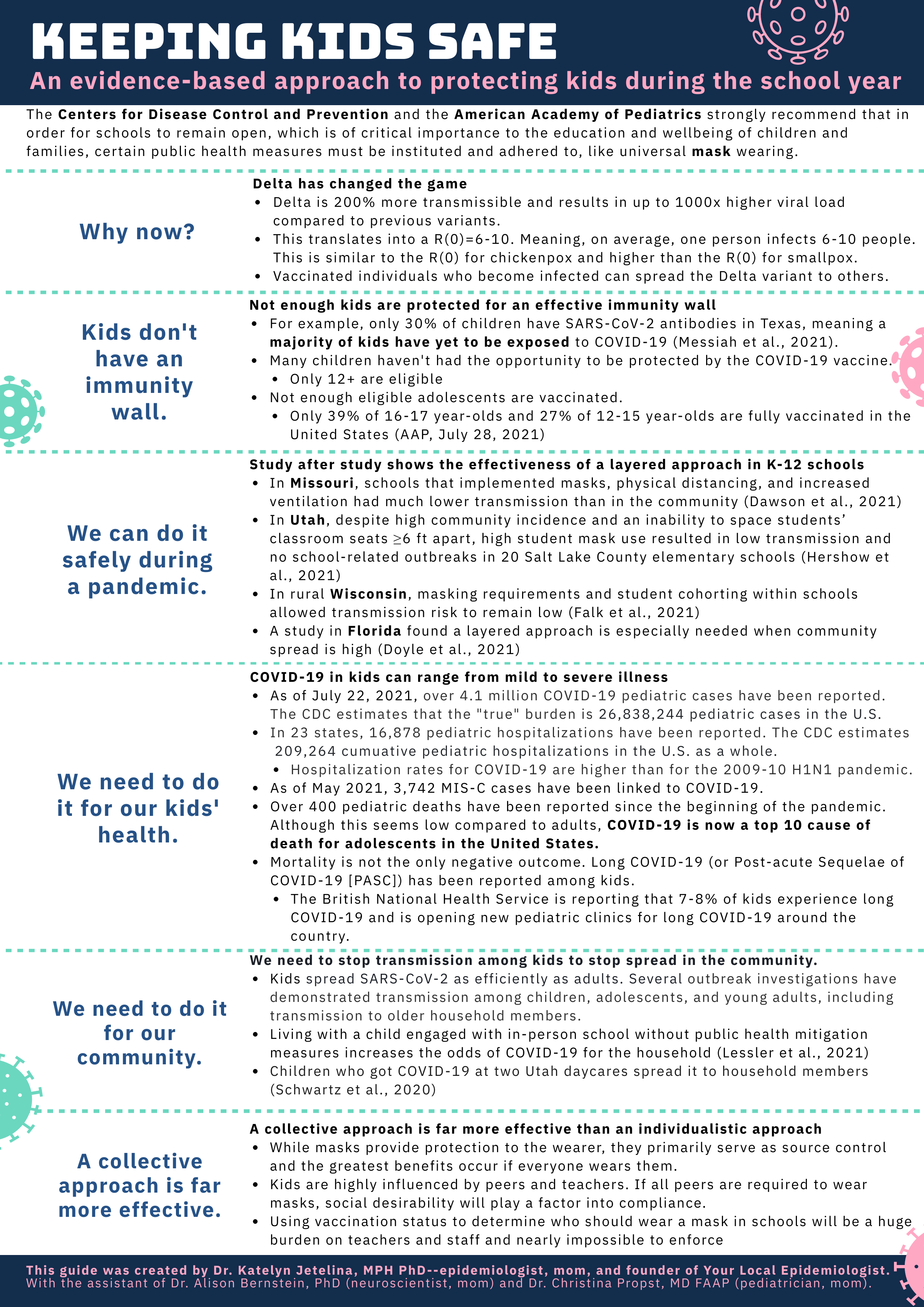
A PDF outlining an evidence-based approach to protecting children during the school year.

Safe, Strong, & Health Schools
Doctors, educators, scientists, and leaders explore ways schools can safely provide in-person learning.

The ABC Science Collaborative
A program that pairs scientists and physicians with school leaders to help understand Covid-19 and school safety.

Wisconsin Department of Health Services (DHS)
Find guidance and resources for caring for Wisconsin children.

Public Health Madison Dane County
Read Public Health Madison Dane County's Fall 2021 Guidance for Dane County K-12 schools.

Restarting Safe Education and Testing (ReSET)
Priorities and resources for a safe return-to-school for children with complex health needs.

UW Health: Covid Vaccines and Kids
Here are some common questions and answers about the Covid-19 vaccines and children.
Impact of Masking in School
| Domains | Fully Masked Environment | “Masks Optional” Environment |
Health and Safety |
|
|
Education |
|
|
Operations |
|
|